

Study screening and common traits of are research
Our systematic overview and meta-analysis initiated with the method of literature search and screening. The PRISMA movement diagram of the included research is offered in Fig. 1.
During the literature screening course of, D.S. took the lead position in making inclusion choices, each on the ‘title and summary stage’ and the ‘full textual content screening stage,’ in session with different researchers. No important disagreement between authors was discovered on this course of. Table S3 lists the research that investigated the associations of our pursuits from sure views but have been excluded resulting from their deviation from our overview’s exact scope, together with the explanations for his or her exclusion.
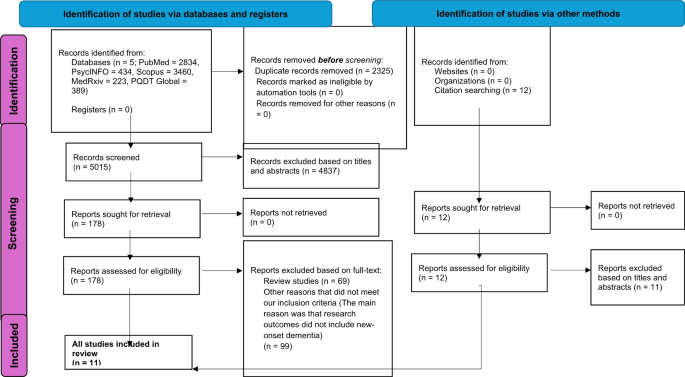
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram demonstrating search technique
This process consequently resulted within the inclusion of knowledge from 939,824 post-COVID-19 circumstances and 6,765,117 controls throughout 11 research [6, 9, 12, 13, 27,28,29,30,31,32,33], as detailed in Table 1. All these research investigated the danger of NOD in older adults with and with out COVID-19 an infection over various observational durations. The general incidence of NOD within the COVID-infected group was round 1.82% (starting from 0.3 to six.4%), whereas the non-COVID-infected group exhibited an incidence of round 0.35% (starting from 0.0 to five.0%), over a median remark interval of 12 months (starting from 3 to 24 months). To interpret, the general incidence was calculated by aggregating the variety of NOD circumstances and the whole variety of people within the COVID-19-infected or non-COVID-infected teams throughout all included research to acquire an averaged incidence. For instance, to calculate the averaged general incidence within the COVID-infected group, we summed the NOD circumstances particularly from the COVID-infected group from every research and divided them by the whole variety of members within the COVID-infected teams. We utilized the identical methodology to calculate the averaged general incidence within the non-COVID-infected group, and the incidence in particular person research. In research reporting incidences for various follow-up durations (e.g., 3, 6, 12, or 24 months), we used the longest obtainable follow-up interval for consistency.
Of be aware, 5 research employed Propensity Score Matching (PSM) to ascertain 1:1 matched cohorts of older adults with out COVID-19, due to this fact making certain comparability of baseline traits between COVID-positive and management teams [12, 27, 28, 30, 32]. The dementia danger within the COVID-positive group was in comparison with two forms of management teams: non-COVID cohorts with different respiratory infections [control group (C1)] [12, 28, 30, 31, 33], and non-COVID cohorts with in any other case unspecified well being standing [control group (C2)] [6, 9, 13, 27, 29, 32, 33]. In addition, whereas 9 research recorded definitive dementia diagnoses utilizing ICD-10, the TICS-40 in Liu et al.‘s research was used to point, quite than affirm, dementia [6, 9]. The focus was on all-cause dementia (primarily together with AD, vascular dementia, and unspecified dementia) in eight research, whereas the remaining three particularly examined AD [13, 32, 33]. In research addressing all-cause dementia, AD was essentially the most prevalent sort (in the event that they reported the proportions of every dementia subtype), adopted by vascular dementia [29, 31]. Refer to Table 1 for extra particulars of different traits.
Quality evaluation
Every research included in our overview was rated nearly as good high quality (≥ 7 stars) based mostly on the NOS high quality evaluation standards [34], as the small print proven in Table S4(a) for 10 cohort research and Table S4(b) for one cross-sectional research (longitudinal in nature with a cross-sectional evaluation). No disagreement concerning the standard appraisal amongst included research between researchers was discovered. The research by Park et al. and Qureshi et al. every misplaced one level for NOS comparability gadgets, as they solely managed for demographic options, however not for identified dementia danger components such because the physique mass index, alcohol consumption, smoking historical past and bodily exercise [29, 30]. The research by Liu et al. in 2021 and 2022 every misplaced one level on the merchandise ‘evaluation of the end result’ as a result of the cognitive standing of the members was self-reported [6, 9]. The research by Zarifkar et al. misplaced two factors on NOS comparability gadgets, resulting from its failure to manage for age, intercourse, and different components [33]. The research by Cohen et al. [27], Liu et al. in 2021 [6], Park et al. [29], and Taquet et al. in 2021 [31], misplaced one level on the NOS consequence gadgets resulting from their failure to supply a follow-up interval of at the least 12 months for outcomes to happen.
Overall pooled meta-analysis outcomes from all 11 included research
In the principle pooled evaluation, the forest plot in Fig. 2 confirmed the variations in NOD dangers between COVID-infected group and non-COVID-infected group throughout the 11 included research. A random-effects REML mannequin was used resulting from substantial heterogeneity. We didn’t distinguish between non-COVID-19 statuses, grouping collectively each wholesome people and people with different forms of respiratory infections as controls. The general pooled evaluation revealed a major hyperlink between COVID-19 an infection and elevated danger for NOD in COVID-19 older grownup survivors (RR = 1.58, 95% CI 1.21–2.08, p < 0.001; I2 = 98.57%, p < 0.001).
Among separate research, 9 out of 11 research reported an elevated danger for creating NOD in COVID-infected older adults, compared to their non-infected counterparts [6, 9, 12, 13, 27, 30,31,32,33]. Notably, in comparison with eight research indicating a RR from 1.28 to 4.87, one research confirmed that COVID-19 an infection led to a probability of creating NOD that was greater than 20 instances that of these uninfected (RR = 20.92, 95% CI 1.29-340.63) [6], albeit contributing minimally to the general weight (0.87%). Zero dementia occasions within the non-COVID-infected group have been reported on this research, which might theoretically lead to an infinite danger ratio [6]. However, the statistical software program addressed this problem in meta-analyses by using a continuity correction. For the research in query, this concerned including a nominal worth of 0.5 to every cell of the two × 2 contingency desk. This adjustment was designed to mitigate the computational difficulties posed by zero occasions and to permit for the estimation of an adjusted danger ratio [35]. The identical approaches have been utilized throughout all meta-analyses, as essential.
In distinction, one research urged no important distinction in NOD danger between COVID-infected and non-infected teams (RR = 1.03, 95% CI 0.83–1.30) [28], whereas one other research by Park et al. urged a protecting impact of COVID-19 an infection in opposition to NOD danger (RR = 0.64, 95% CI 0.48–0.86) [29]. However, we observed that this danger ratio (i.e., 0.64) was calculated by us with out contemplating confounding covariates. In their unique article [29], a constantly increased danger of NOD in COVID-infected people was noticed throughout all age teams of their fashions adjusted for a number of covariates. Therefore, it may be inferred that, had changes for confounding components been attainable (which weren’t carried out by us resulting from inaccessible related information), COVID-19 an infection might nonetheless be related to an elevated NOD danger amongst older grownup survivors in our evaluation.
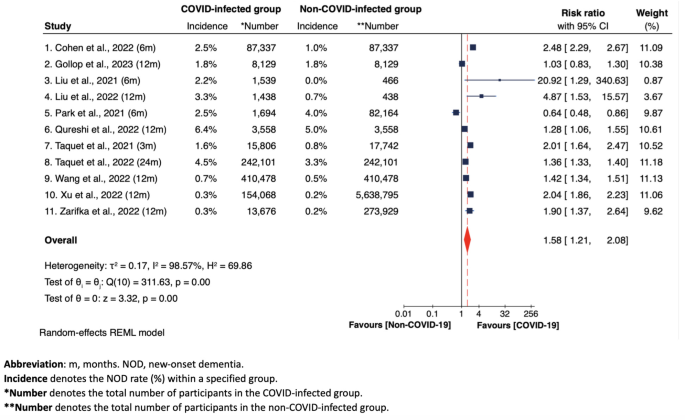
Forest plot of general pooled meta-analysis of NOD danger between COVID-infected group and non-COVID-infected group throughout all 11 research
Subgroup analyses
Figures 3, 4 and 5, together with Supplementary Figures S1 to S5, show the outcomes of subgroup analyses, analyzing: (i) NOD danger solely based mostly on observational durations (i.e., at 3, 6, 12, 24 months) (Fig. 3); (ii) NOD danger based mostly on COVID-19 an infection standing [infected vs. other respiratory infections (C1) (Fig. 4), and infected vs. uninfected (C2) (Fig. 5)]; (iii) danger of creating cognitive impairment in COVID-infected group in comparison with non-COVID-infected group (right here C1 and C2 have been grouped collectively), with cognitive impairment (together with each CIND and dementia circumstances) because the measured consequence (Figure S1); (iv) NOD danger throughout three teams – these testing constructive for COVID-19, these with different respiratory infections, and people testing unfavourable for COVID-19 in any other case unspecified, particularly based mostly on intercourse variations (Figure S2); and (v). NOD danger amongst COVID-19 sufferers, categorized by COVID-19 severity (Figure S3 and S4); and (vi) NOD danger between COVID-infected and non-COVID-infected teams amongst research using propensity-score matching method (Figure S5). Most of those subgroup meta-analyses utilized random-effects REML fashions resulting from substantial heterogeneity.
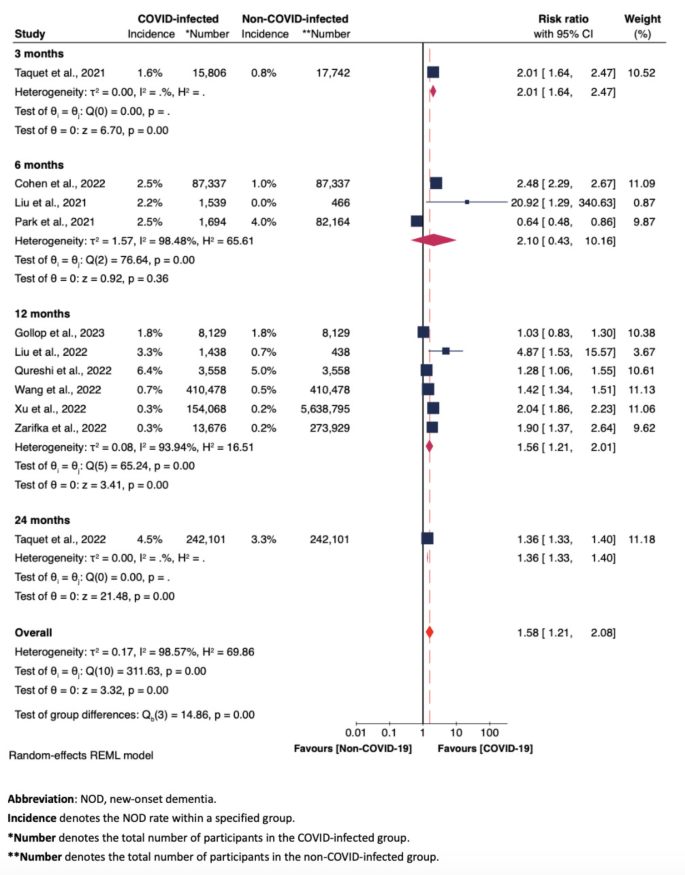
Forest plot of the meta-analysis of NOD danger between COVID-infected group and non-COVID-infected group at 3, 6, 12, 24 months, involving all 11 research

Forest plot of the meta-analysis of NOD danger between COVID-infected group and C1 group at 3, 6, 12, 24 months

Forest plot of the meta-analysis of NOD danger between COVID-infected group and C2 group at 3, 6, 12, 24 months
NOD danger amongst COVID-infected and non-COVID-infected teams, based mostly on observational durations
Figure 3 illustrates that, when analyzing pooled outcomes from a couple of particular person research, the danger ratio at 12 months was considerably better within the group contaminated with COVID-19 (RR = 1.56, 95% CI 1.21–2.01), carefully aligning with the general pooled danger ratio in Fig. 2 (RR = 1.58, 95% CI 1.21–2.08). Also, this subset displays lowered heterogeneity (I2 = 93.94%, Fig. 3) compared to the broader evaluation of all 11 research (I2 = 98.57%, Fig. 2). However, the rise in danger ratio at six months was not statistically important (RR = 2.10, 95% CI 0.43–10.16). This lack of significance could be attributed to the outlier danger ratio of 0.64 reported by Park et al., which was a price earlier than adjustment [29].
NOD danger amongst COVID-Infected, non-COVID-infected in any other case unspecified, and non-COVID-infected with different respiratory infections teams throughout follow-up durations
Figure 4 exhibits no exceptional distinction about NOD danger between the COVID-19 group and the non-COVID cohorts with different respiratory infections [C1 group] (general RR = 1.13, 95% CI 0.92–1.38). Figure 5 exhibits a considerably elevated danger for NOD within the COVID-19 group in comparison with the non-COVID cohorts with in any other case unspecified well being statuses [C2 group] at 12 months post-COVID-19 (RR = 1.84, 95% CI 1.41–2.38). This elevated danger was not evident at three months (RR = 0.87, 95% CI 0.46–1.65) or six months (RR = 1.73, 95% CI 0.72–4.14). Here the shortage of statistical significance at six months can be attributed to the consequence from Park et al. [29], which, as soon as adjusted, might contribute to an general important enhance in NOD danger at six months.
Comparison of newly developed cognitive impairment danger between COVID-infected and non-COVID-infected teams
Figure S1 exhibits that, among the many 3 research which explored the danger of creating new-onset cognitive impairment between the COVID-Infected and the non-COVID-infected teams [6, 9, 27], a major elevated danger for NOD was noticed within the COVID-infected group (general RR = 1.93, 95% CI 1.52–2.43, p < 0.001; I2 = 79.04%, p < 0.001). In different phrases, cognitive impairment was practically twice as doubtless in COVID-19 older grownup survivors in comparison with these with out COVID-19 an infection.
NOD danger based mostly on intercourse in COVID-positive, different respiratory an infection, and COVID-negative in any other case unspecified teams, individually
Notably, Figure S2 exhibits increased NOD dangers for ladies on each the COVID-positive group (RR = 1.65, 95% CI 1.53–1.78, p < 0.001; I2 = 0.00%, p > 0.05) and COVID-negative in any other case unspecified management group (RR = 1.33, 95% CI 1.22–1.44, p < 0.001; I2 = 0.00%, p > 0.05), indicating that COVID-19 an infection itself was not a significant underlying issue making ladies extra inclined to creating NOD in contrast with males.
NOD danger amongst COVID-infected sufferers, based mostly on COVID-19 severity (inpatient vs. outpatient)
Both Figures S3 and S4 present considerably increased dangers for NOD amongst COVID-infected older grownup outpatients (RR = 1.91, 95% CI 1.06–3.45) and inpatients (RR = 3.06, 95% CI 2.78–3.37), as in comparison with COVID-negative older adults.
NOD danger between COVID-infected and non-COVID-infected teams, based mostly on research with propensity rating matching (PSM)
Figure S5 signifies that the one 5 research utilizing PSM reported an elevated NOD danger within the COVID-infected group (Overall RR = 1.46, 95% CI 1.10–1.94) [12, 27, 28, 30, 32]. This enhance in NOD danger is in step with the findings from our major evaluation, which incorporates all 11 research (Overall RR = 1.58, Fig. 2).
Overall heterogeneity and sensitivity analyses
We noticed substantial heterogeneity among the many 11 included research in our major general pooled meta-analysis in Fig. 2 (I2 = 98.57%, p < 0.001). Also, L’Abbé and Galbraith plots, as proven in Figure S6 and Figure S7, visually point out the discrepancies amongst these research. Contrary to expectations, the meta-regression outcomes, as proven in Figure S8, recommend that covariates akin to observational durations (3, 6, 12, 24 months), forms of management teams (non-COVID cohorts in any other case unspecified vs. non-COVID cohorts with different forms of respiratory infections), and dementia sorts assessed (all-cause dementia vs. AD) didn’t contribute to the variability among the many 11 research. The sensitivity evaluation, as proven in Figure S9, means that the general outcomes remained constant regardless of the elimination of every particular person research (with acceptable modifications in impact measurement starting from 0.09 to 0.12), indicating that the findings of our major meta-analysis in Fig. 2 have been strong and never overly depending on any single research.
Publication bias
The contour-enhanced funnel plot, illustrated in Figure S10, visually signifies potential asymmetry, hinting at publication bias. Two imputed research have been strategically positioned to reflect the asymmetrical gaps. However, the regression-based Egger’s check (p = 0.052) and the nonparametric rank correlation Begg’s check (p = 0.978) don’t present sturdy proof of serious publication bias in our major general pooled meta-analysis. Meanwhile, incorporating the 2 imputed research into the evaluation yields a revised pooled impact measurement for a complete of 13 research (RR = 1.48, 95% CI 1.12–1.96), which nonetheless doesn’t markedly differ from the preliminary evaluation (RR = 1.58, 95% CI 1.21–2.08). In addition, the typical high quality appraisal (NOS) rating of 8.1 [standard deviation (SD) = 0.79] is suggestive of a superb methodological high quality of the 11 included research. All included research correctly symbolize the goal inhabitants, investigating the influence of COVID-19 on the NOD danger in older adults, with passable pattern sizes all through.



{kind=link}